Example Cms 1500 Form Filled Out. Check with the relevant MAC for details.
 2012 2021 Form Cms 1500 Fill Online Printable Fillable Blank Pdffiller
2012 2021 Form Cms 1500 Fill Online Printable Fillable Blank Pdffiller
Download CMS Claim Form 1500 which is used by health care professionals to bill Medicare and Medicaid.

Cms 1500 form sample. Example of an individual NPI reporting on a single CMS-1500 claim for 2013 Physician Quality Reporting System PQRS. Our CMS 1500 form PDF downloadable is simple to use and comes as a blank CMS 1500 claim form PDF. The NUCC has developed this general instructions document for completing the 1500Claim Form.
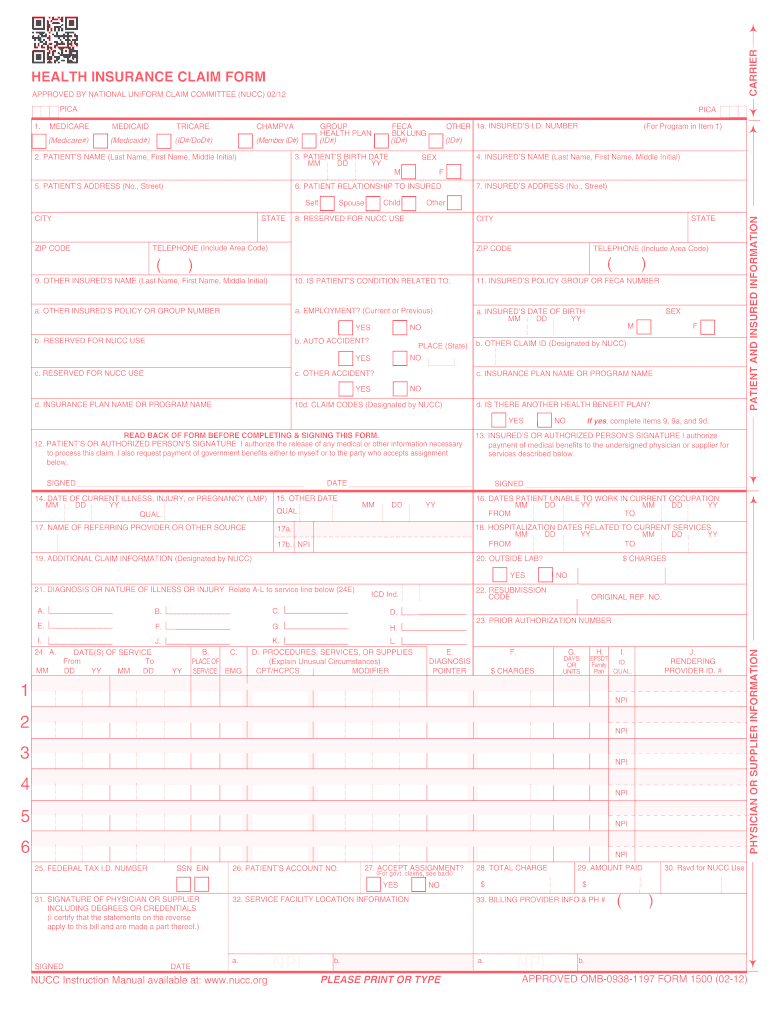
PLEASE PRINT OR TYPEAPPROVED OMB-0938-1197 FORM 1500 02-12 APPROVED OMB-0938-1197 FORM 1500 02-12 1a. Sample Revised CMS 1500 Form rev. Add an e-signature by typing or drawing with your touchpad.
The 1500 Health Insurance Claim Form 1500 Claim Form is in the public domain. 21 Posts Related to Sample Cms 1500 Form Filled Out. Hcfa 1500 Claim Form Sample.
Sample form Information and Instructions for Form CMS-1500 0212 for all insurance companies. Example Of 1500 Claim Form Filled Out. Sample Cms 1500 Form Filled Out Pdf.
The provider is reporting several measures related to diabetes coronary artery disease CAD and urinary incontinence. November 29 2018 by Jerry. Sample 1500 Claim Form Filled Out.
This will make checking process easier since the insurance company will be able to know when the practice occurs. T his address is for comments andor suggestions only. If you have any comments concerning the accuracy of the time estimates or suggestions for improving this form please write to.
Cms 1500 Claim Form Sample. Sample Cms 1500 Form Filled Out. Until March 31 2014 one can use either the old CMS-1500 claim form version 0805 as marked in the lower right hand corner or the new CMS-1500 version 0212 for paper claims submitted to Medicare BCBS and BHS.
ZINPLAVA bezlotoxumab for Injection 25 mgmL Some Medicare Administrative Contractors may want you to record the total number of vials used. INSUREDS ADDRESS No Street CITY STATE ZIP CODE TELEPHONE Include Area Code 11. The form is used by Physicians and Allied Health Professionals to submit claims for medical services.
02-12Physician Office Box 24G Units Administration J0178 has a unit descriptor of 1 mg. Completed Cms 1500 Claim Form Sample. In addition to Medicare parts AB and for Medicare durable medical equipment Administrative Contractors.
Sample Cms 1500 Claim Form Completed. You may also upload your signature from your device. The date when patient receives your medical service must be documented on sample CMS 1500 form that you fill.
SA M PL E PLEASE PRINT OR TYPE APPROVED OMB-0938-1197 FORM 1500 02-12. The CMS 1500 form has to be signed by both the claimer and the physician or supplier in order to certify that the services listed in the document were medically indicated and necessary for the health of the patient. This CMS 1500 form fillable and simple to use is available to anyone who needs it.
It is available in various formats eg single copy duplicate etc. The From date is the date of admission and the To date is the discharge date. Sample 1500 Claim Form.
Sample Cms 1500 Form Filled Out. SA M PL E. CMS-1500 Claim PQRS Example.
Sample CMS-1500 Health Insurance Claim Form Created Date. The patient was seen for an office visit 99213. The CMS-1500 02-12 claim form specifications require red drop out ink in order to facilitate the use of image processing technology such as Optical Character Recognition OCR facsimile transmission and image storage.
Sample 1500 Claim Form Filled Out. This document is intended to be a guide for completing the 1500 Claim Form and not definitive instructions for this purpose. Sample Completed 1500 Claim Form.
Instructions for Completing the CMS 1500 Claim Form The Center of Medicaid and Medicare Services CMS form 1500 must be used to bill SFHP for medical services. Our government-approved free fillable CMS 1500 template makes your lives a little bit easier. Box 24D Product Code Enter HCPCS code J0178 to represent EYLEA aflibercept Injection.
Report 2 units of the code when billing for a 2 mg injection of EYLEA. Claims must be made within 12 months after services are provided. It is also used for billing of some Medicaid State Agencies.
Enter t he hospitalization dates related to an inpatient stay in MMDDYY format. CMS-1500 Claim Form Completion for PROMISe Mental Health Substance Abuse Providers Provider Handbook CMS-1500 January 05 2018 1 Purpose of the document The purpose of this document is to provide a block-by-block reference guide to assist the following provider types in successfully completing the CMS-1500. The CMS-1500 form is the standard claim form used by a non-institutional provider or supplier to bill Medicare carriers and durable medical equipment regional carriers DMERCs.
INSUREDS NAME Last Name First Name Middle Initial 7. All items must be completed unless otherwise noted in these instructions. PRA Reports Clearance Officer 7500 Security Boulevard Baltimore Maryland 21244-1850.
Sample CMS-1500 Claim Form for Office Billing. Sample Cms 1500 Claim Form. Medicare Part B Cms 1500 Claim Form Instructions.
Any user of this document should refer to the most. NUMBER For Program in Item 1 4.



